
The clinical course of monoclonal gammopathies
|
The life expectancy of symptomatic patients has been improved by the introduction of high-dose melphalan (Alkeran°), the contribution of new drugs (in particular thalidomide then its derivative lenalidomide (Revlimid°) and bortezomib), and better clinical management of the complications of the disease (particularly bone complications, through the use of osteoclast inhibitors and bisphosphonates). Nevertheless, myeloma remains an incurable disease. Waldenström’s macroglobulinaemia has a more chronic clinical course, especially with treatment, the main drugs being chlorambucil, rituximab and fludarabine. |
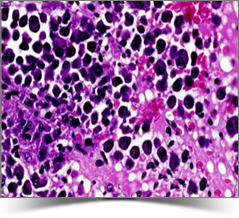 Histological examination of bone marrow infiltrated by abnormal plasma cells |
The clinical course of MGUS has been investigated in studies, the largest of which involved more than 1300 patients with variable levels of monoclonal Ig up to 30 g/L of IgG (two-thirds of subjects), IgA or IgM class. Spontaneous disappearance of the monoclonal Ig was only rarely observed over a very long follow-up period (median: 15 years) and only occurred in patients with very low Ig levels. The risk of progression to overt myeloma or a related disease was estimated to be about one percent per year. This risk does not increase over time but persists for many years after detection of the monoclonal Ig. The initial concentration of the monoclonal Ig and its type are the main predictors, high levels, IgM and IgA being associated with a higher risk of progression. However, reduced levels of normal polyclonal Igs and the presence of light chains in urine (Bence Jones protein) have no obvious prognostic significance. Measuring the concentration of free light chains in serum for the purposes of risk assessment is of limited value, and it is questionable whether this test should be performed routinely.
The risk of about one percent per year that MGUS will progress to myeloma or a related disorder warrants regular long-term monitoring. The main monitoring investigation is serum protein electrophoresis, which is much more reliable for assessing changes in monoclonal Ig levels than measuring Ig concentrations. Standard laboratory parameters (when the monoclonal Ig is an IgG or IgA, full blood count, serum creatinine, serum calcium and urinary protein) should also be checked. However, monitoring serum levels of free light chains is almost never indicated in this situation. Additional investigations (e.g. bone marrow differential count, skeletal radiography) are only justified if clinical or laboratory parameters change, particularly if the monoclonal Ig level increases, which is to be considered a reliable « tumour marker ». The monitoring frequency depends on the context. It is usually preferable to repeat the main tests about 3 months after detection of the gammopathy. Thereafter, when all the data unambiguously suggest the diagnosis of MGUS, twice-yearly monitoring is sufficient (or annually if the Ig concentration is low). No treatment is indicated and chemotherapy should only be considered if overt progressive disease develops.